Schizophrenia, Circuits, and the Case for Neuromodulation
In schizophrenia, the gap between what we know and what we can treat is wide. While dopamine-blocking drugs help with positive symptoms like delusions and hallucinations, they often leave patients stuck—disengaged, cognitively flattened, and unable to rejoin their lives. These are not just medication side effects. They reflect a deeper circuit-level pathology we’ve yet to fully grasp, let alone treat.
That’s why a recent study from Johns Hopkins University on deep brain stimulation (DBS) in treatment-resistant schizophrenia (https://www.medrxiv.org/content/10.1101/2025.04.09.25325419v1) is important.
From the Basal Ganglia to the Mediodorsal Thalamus
Most neurostimulation studies in schizophrenia have chased symptoms by targeting structures downstream: the nucleus accumbens, anterior cingulate, habenula. The Hopkins group tried something different. They went upstream.
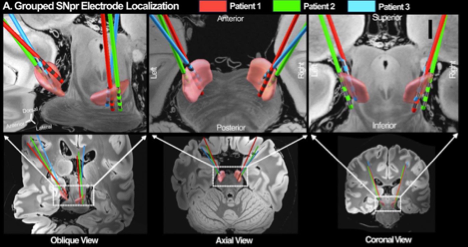
Their target was the substantia nigra pars reticulata (SNpr)—a GABAergic output nucleus of the basal ganglia—and their hypothesis was bold: by stimulating SNpr, they could indirectly normalize activity in the mediodorsal thalamus (MD), which then projects to prefrontal areas involved in internal narrative, belief evaluation, and cognitive flexibility.
This is the same MD thalamus our lab has studied for over a decade—an area that helps prefrontal cortex update inferences based on context. It’s a structure we believe sits at the heart of psychosis: when it fails, belief updating can go haywire, creating fixed delusions or disordered thought.
In the Hopkins study, the researchers observed that relief from auditory verbal hallucinations (AVH) correlated with stimulation sites that were structurally connected to the angular gyrus, precuneus, and supramarginal gyrus, and functionally connected to the MD thalamus, orbitofrontal cortex, and dorsolateral PFC. In other words: the circuit matters. It’s not about shutting down one region. It’s about recalibrating a distributed network.
Why This Matters
The implications are profound. First, it reorients DBS in schizophrenia away from crude anatomical targets and toward network-informed precision. Second, it reinforces the idea that symptoms like hallucinations emerge not from hyperactive “voice centers,” but from failures in higher-order control—failures of gating, updating, and internal monitoring.
It’s also a reminder that the basal ganglia-thalamocortical loop, long studied in motor and motivational systems, may be just as central to psychosis. And importantly, it opens the door to interventions that don’t rely on blocking dopamine—interventions that might actually re-enable learning in brains locked into maladaptive internal narratives.
Non-Invasive Options: The Road Ahead
Of course, DBS isn’t scalable for most patients. But the logic behind it—targeting circuits, not just symptoms—extends to non-invasive tools.
Transcranial Magnetic Stimulation (TMS) has been used to target dorsolateral PFC in negative symptom treatment, with modest but real results. Theta-burst TMS and deep TMS aim to access deeper or more complex circuits, but their effects remain variable.
More recently, focused ultrasound (tFUS) has emerged as a way to non-invasively stimulate deep brain structures—including the thalamus. Preclinical studies suggest tFUS can alter prefrontal-striatal-thalamic dynamics in animal models of schizophrenia. In principle, it could access hubs like the MD thalamus or even modulate the same nigrothalamic loops targeted by DBS, without surgery.
From Circuits to Computation
All of this underscores a broader shift: away from neurotransmitters as endpoints, and toward circuit-level computation. The brain isn’t just a set of chemical gradients. It’s a machine that builds models of the world and updates them based on surprise.
Psychosis, then, may not reflect excessive dopamine as much as faulty inference: a thalamus that fails to signal uncertainty, a cortex that overcommits to priors, a basal ganglia that no longer weighs competing predictions.
Neuromodulation—whether invasive or not—offers a way to restore the computational dialogue between regions, to re-enable plasticity rather than dampen symptoms. And it pushes psychiatry toward a future where interventions are judged not just by where they act, but how they change the brain’s ability to learn.